Antimicrobials
3.7 Cephalosporins
Open Resources for Nursing (Open RN)
Cephalosporins are a slightly modified chemical “twin” to penicillins due to their beta-lactam chemical structure. (See Figure 3.8 for a comparison of the beta-lactam ring structure, spectrum of activity, and route of administration across different classes of medications.) Because of these similarities, some clients who have allergies to penicillins may experience cross-sensitivity to cephalosporins.

Indications for Use: Cephalosporins are used to treat skin and skin-structure infections, bone infections, genitourinary infections, otitis media, and community-acquired respiratory tract infections.
Mechanism of Action: Cephalosporins are typically bactericidal and are similar to penicillin in their action within the cell wall. Cephalosporins are sometimes grouped into “generations” by their antimicrobial properties. The 1st-generation drugs are effective mainly against gram-positive organisms. Higher generations generally have expanded spectra against aerobic gram-negative bacilli. The 5th-generation cephalosporins are active against methicillin-resistant Staphylococcus aureus (MRSA) or other complicated infections. [1]
Nursing Considerations Across the Lifespan: Most cephalosporins are considered safe for use in pediatrics. Some dose adjustments are required based on renal dysfunction in older adults. Cephalosporins can be given during pregnancy.
Specific Administration Considerations: Clients who are allergic to pencillins may also be allergic to cephalosporins. Clients who consume cephalosporins while drinking alcoholic beverages may experience disulfiram-like reactions including severe headache, flushing, nausea, vomiting, etc.[2] Additionally, like penicillins, cephalosporins may interfere with coagulability and increase a client’s risk of bleeding. Cephalosporin dosing may require adjustment for clients experiencing renal impairment. Blood urea nitrogen (BUN) and creatinine should be monitored carefully to identify signs of nephrotoxicity.
Client Teaching & Education: Clients who are prescribed cephalosporins should be specifically cautioned about a disulfiram reaction, which can occur when alcohol is ingested while taking the medication. Additionally, individuals should be instructed to monitor for rash and signs of superinfection (such as black, furry overgrowth on tongue; vaginal itching or discharge; loose or foul-smelling stool) and report to the prescribing provider.
It is also important to note that cephalosporin can enter breastmilk and may alter bowel flora of the infant. Thus, use during breastfeeding is often discouraged.[3]
Now let’s take a closer look at the cephalosporin medication card in Table 3.6.[4] Because information about medication is constantly changing, nurses should always consult evidence-based resources to review current recommendations before administering specific medication.
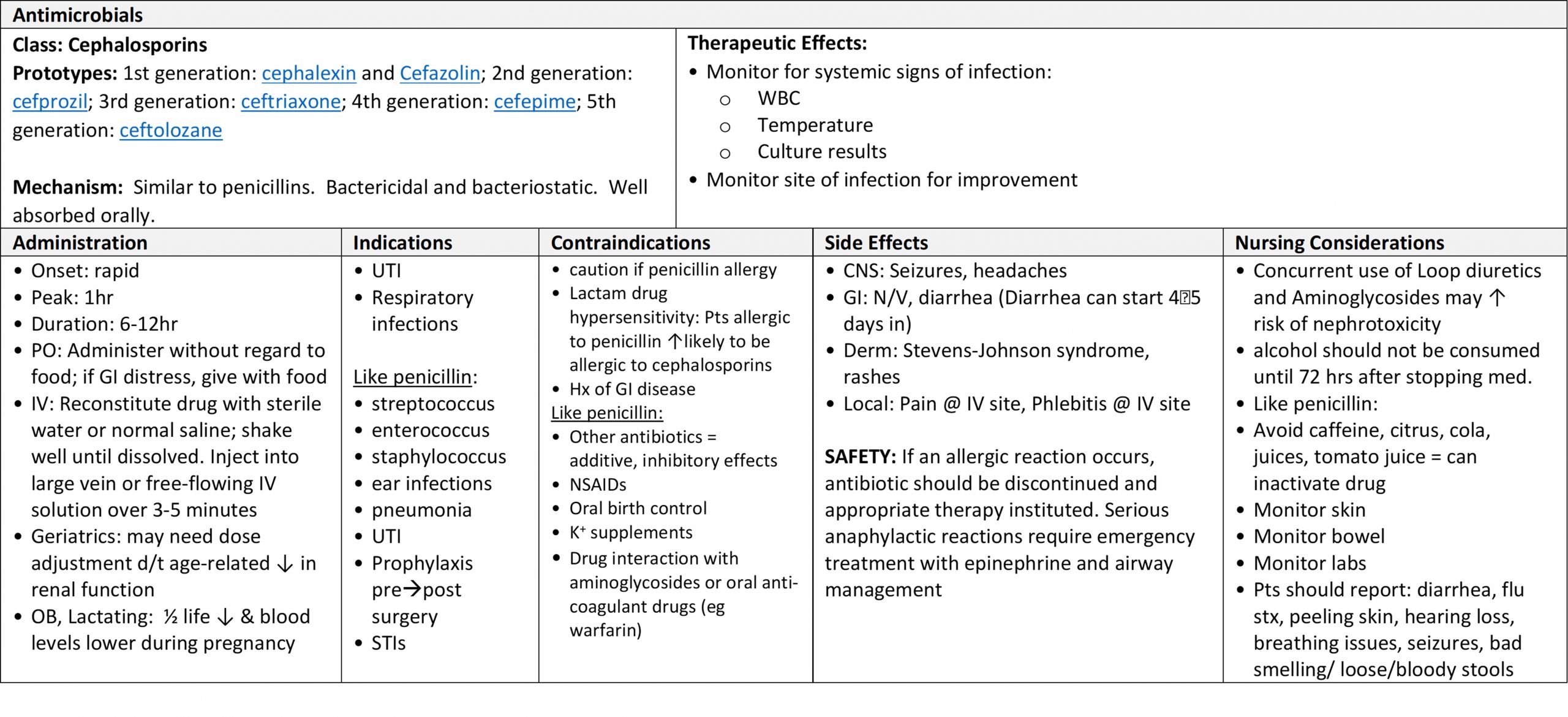
Table 3.6 Cephalosporin Medication Card [5]
Class: Cephalosporins (prototypes: 1st generation: cephalexin and cefazolin; 2nd generation: cefprozil; 3rd generation: ceftriaxone; 4th generation: cefepime; 5th generation: ceftolozane).
Clinical Reasoning and Decision-Making Activity 3.6a
Using the above grid information, consider the following clinical scenario question:
Mrs. Jenkins is an 89-year-old client admitted to the medical-surgical floor for treatment of a skin infection. The admitting provider prescribes Cefazolin 1 gram every 8 hours IV.
Mrs. Jenkins’ admission laboratory tests include renal laboratory studies reflecting:
Creatinine: 120 μmol/L (Normal range: 50-110 μmol/L[6]
Blood urea nitrogen (BUN): 10.5 mmol/L (Normal: 2.9-8.2 mmol/L)
Glomerular Filtration Rate: 55 ml/min (Normal: 90-120 ml/min)[7]
On Day 3 Mrs. Jenkins has renal laboratory studies performed again. The results are:
Creatinine: 150 μmol/L
Blood urea nitrogen (BUN): 16.8 mmol/L
Glomerular Filtration Rate: 20 ml/min
Are Day 3 findings expected or not? What course of action should the nurse take?
Note: Answers to the activities can be found in the “Answer Key” sections at the end of the book.
Media Attributions
- cephalosporins
- Werth, B.J. (2018, August). Cephalosporins. Merck Manual Professional Version. https://www.merckmanuals.com/professional/infectious-diseases/bacteria-and-antibacterial-drugs/cephalosporins ↵
- Ren, S., Cao, Y., Zhang, X., Jiao, S., Qian, S., & Liu, P. (2014). Cephalosporin induced disulfiram-like reaction: a retrospective review of 78 cases. International Surgery, 99(2), 142–146. https://www.internationalsurgery.org/doi/full/10.9738/INTSURG-D-13-00086.1 ↵
- uCentral from Unbound Medicine. https://www.unboundmedicine.com/ucentral ↵
- Daily Med, https://dailymed.nlm.nih.gov/dailymed/index.cfm, used for hyperlinked medications in this module. Retrieved June 27, 2019. ↵
- UpToDate (2021). Cefazolin. https://www.uptodate.com/contents/search ↵
- U.S. National Library of Medicine, Medline Plus. (2020, February 13). Basic metabolic panel. https://medlineplus.gov/ency/article/003462.htm ↵
- U.S. National Library of Medicine, Medline Plus. (2020, February 13). Glomerular filtration rate. https://medlineplus.gov/ency/article/007305.htm ↵
