Ankyloglossia, also known as tongue-tie, is a congenital oral condition that can cause difficulty with breastfeeding, speech articulation, and mechanical tasks such as licking the lips. The term tongue-tie comes from an unusually short membrane (the frenulum) attaching the tongue to the floor of the mouth. There are different types of tongue tie, defined by where the tissue restricting movement is attached. Anterior tongue tie is more common, but it is also possible for an infant to have a posterior tongue tie.
Tethered oral tissues (TOTs) refers to restrictive tissue in the mouth that impacts how you are able to use your mouth. The presence of a piece of tissue (frenulum) under the tongue, lips or around the cheeks does not mean someone is “tied”. A true tie affects the function of your body.
Awareness of this subject has grown dramatically. We are now seeing so many tongue-tied patients reaching out on their own.
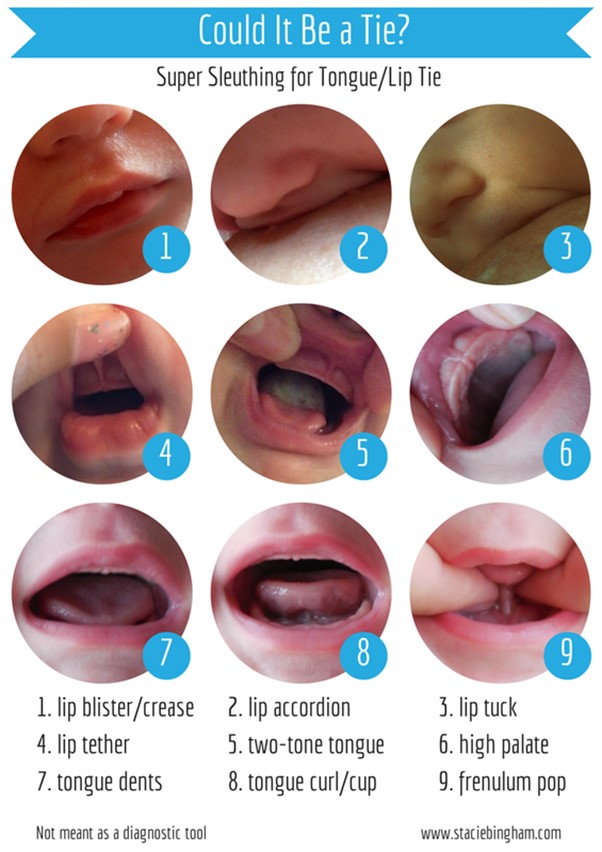
Signs and symptoms of tongue-tie include:
• Difficulty lifting the tongue to the upper teeth or moving the tongue from side to side
• Trouble sticking out the tongue past the lower front teeth
• A tongue that appears notched or heart shaped when stuck out
See a dentist / lactation consultant if:
• Your baby has signs of tongue-tie that cause problems, such as having trouble breast-feeding
• A speech-language pathologist thinks your child’s speech is affected by tongue-tie
• Your older child complains of tongue problems that interfere with eating, speaking or reaching the back teeth
• You’re bothered by your own symptoms of tongue-tie
Causes
Typically, the lingual frenulum separates before birth, allowing the tongue free range of motion. With tongue-tie, the lingual frenulum remains attached to the bottom of the tongue. Why this happens is largely unknown, although some cases of tongue-tie have been associated with certain genetic factors.
Risk factors
Although tongue-tie can affect anyone, it’s more common in boys than girls. Tongue-tie sometimes runs in families.
Complications
Tongue-tie can affect a baby’s oral development, as well as the way he or she eats, speaks and swallows.
For example, tongue-tie can lead to:
• Breast-feeding problems. Breast-feeding requires a baby to keep his or her tongue over the lower gum while sucking. If unable to move the tongue or keep it in the right position, the baby might chew instead of suck on the nipple. This can cause significant nipple pain and interfere with a baby’s ability to get breast milk. Ultimately, poor breast-feeding can lead to inadequate nutrition and failure to thrive.
• Speech difficulties. Tongue-tie can interfere with the ability to make certain sounds — such as “t,” “d,” “z,” “s,” “th,” “r” and “l.”
• Poor oral hygiene. For an older child or adult, tongue-tie can make it difficult to sweep food debris from the teeth. This can contribute to tooth decay and inflammation of the gums (gingivitis). Tongue-tie can also lead to the formation of a gap or space between the two bottom front teeth.
• Challenges with other oral activities. Tongue-tie can interfere with activities such as licking an ice cream cone, licking the lips, kissing or playing a wind instrument.
Treatment for Tongue Tie
Treatment for a tongue tie ranges from a “wait-and-see” approach to immediate surgical correction. It is possible for the tongue tie to loosen up and relax with time. But some doctors prefer to prevent any possible eating or speech issues by treating the problem before the baby goes home for the first time.
One of the most common surgical treatments is a procedure called a frenotomy. One study published in the International Journal of Pediatric Otorhinolaryngology found that 85 percent of patients who had the procedure showed an immediate improvement in their ability to breastfeed. During a frenotomy, the doctor cuts the frenulum — the band of tissue that connects the tongue to the bottom part of the mouth. Often, a frenotomy is such a quick and easy procedure that it requires no anaesthetic.
If your infant is having trouble breastfeeding, or your older child is developing speech difficulties, schedule a visit with your dentist to confirm or rule out a posterior tongue tie. Since a posterior tie can be difficult to detect, getting the opinion of a medical professional can help you figure out what steps to take next.
Most often parents come to us after the diagnosis of a tongue or a lip tie with the thought process that a simple procedure will suddenly change the way their baby breastfeeds. Well that is the case BUT it requires a lot of Pre and Post treatment follow-up along with a team approach where the baby is evaluated holistically.
Teamwork to evaluate and treat babies with tongue ties is the key to a successful procedure.
The body is a very good communicator, if we listen to it! The body is also very resilient and it will usually figure out a way to perform when we ask it to. Babies come with certain reflexes right from birth. But sometimes a new born baby with oral restrictions such as ties can have latching issues while nursing which is discomforting to the baby and the new mum. Since your newborn has a tongue/lip tie and cannot make use of full range motion of the tongue or lip he/she will start compensating by using his/her muscles of face, chin, lips, jaw or neck to withdraw milk. This muscular compensation leads to discomfort, pain and struggles during a mother’s breastfeeding journey as the tongue’s job is done by other muscles.
If you can listen to it, try to figure out what is going on, and correct it, you can help!
This is because our bodies are beautifully made to compensate and adapt to restrictions in order to carry out the function.
Compensation patterns will only work for so long before something breaks down. Just like if your right leg is injured, your body will compensate to perform walking making more use of the left leg. But it will allow you to walk comfortably only until the left leg starts showing injury due to compensation.
If you have any of the compensation patterns present, it’s a good idea to talk to the lactation consultant trained for identifying tongue tie and its compensations to try and figure out what the underlying problem is.
WHY DO WE REQUIRE A TEAM APPROACH ?
Tongue-tied babies often show some tightness in their body postures, early fusion of the cranial bones, lack of control of the neck muscles or some lack of coordination of the nerves that control the sucking, swallowing and breathing. Often, there is significant muscular discoordination and habit that doesn’t allow them to nurse efficiently. Therefore you may see a change but you will have to give your baby and yourself time to re-adapt and may require help from a trained and certified lactation consultant (IBCLC) and body workers pre and post the frenectomy/frenotomy procedure.
This happens because your baby may have adapted to the compensatory mechanisms to deal with the nursing challenges and a sudden release may create confusion to your baby. Therefore it is absolutely necessary for your baby to undergo the suck retraining and some bodywork inorder to adapt to the changes.
Another way of understanding this is – you met with an accident, suffered from multiple injuries. Your surgeon fixed you up and you were ready to go but were still recommended physical therapy.WHY?
This is because you needed to undergo rehabilitation for your injuries and make sure after the surgery your muscle- balance -posture is retrained. Releasing a tongue tie is also very similar!
When communicating with moms pre-treatment, we cannot stress enough the importance of post treatment care and continued lactation support following the frenectomy procedure. Essentially, the baby must learn how to use his or her tongue in a new way. Some babies need no help at all and immediately breastfeed post-procedure, while other babies may need help from additional professionals.
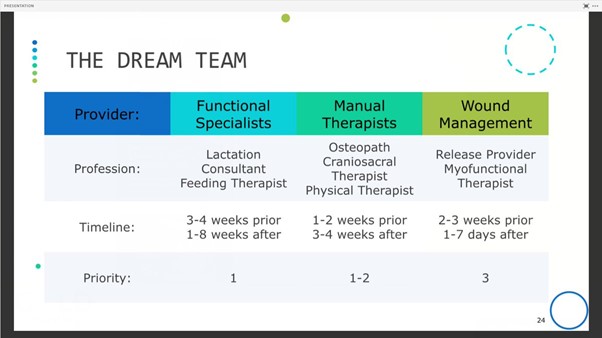
1. Lactation consultant (IBCLC / SACLC) : provides full feeding observation, latch/ position adjustment, suck assessment, pre and post feeding weight checks and strategies for correcting problems and managing breastfeeding.
2. Body workers (craniosacral therapist, osteopath, chiropractor, occupational or physical therapist) : Can help babies to release tight muscles that have compensated for a tight frenulum or improper suck. Bodywork encourages an infant to express postural reflexes and explore natural movement inclinations through the nervous system.
3. A speech or developmental feeding therapist: can help babies learn to use their tongues for more effective eating and speech.
BENEFITS OF HAVING A TEAM APPROACH
A multidisciplinary team approach combines collective expertise from different healthcare professionals to accurately diagnose, comprehensively treat the myriad of tongue ties.
They all come together to solve all problems related to tongue ties like breastfeeding, breathing and sleep patterns, jaw growth and speech issues.
Their focus is not just on the procedure but to improve the breastfeeding journey of the mum and take care of the overall development of the child.
We stress emphasis on having a team approach. Every member of our team is dedicated to advancing the standards of care through learning and applying new pathfinding research, offering advanced education and most importantly caring for the patients’ wellness.
As quoted by Ann Douglas
” If it takes a village to raise a child, it takes a village to support that child’s parent.”
We are here to support you and your baby. Please feel free to Contact Us for any help or assistance.
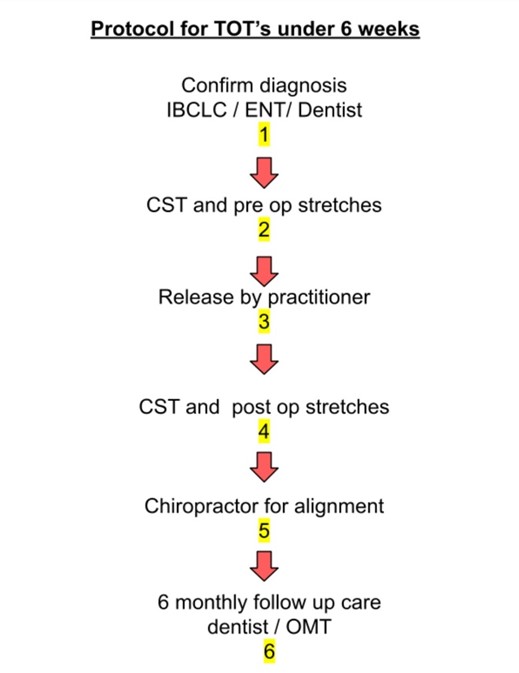
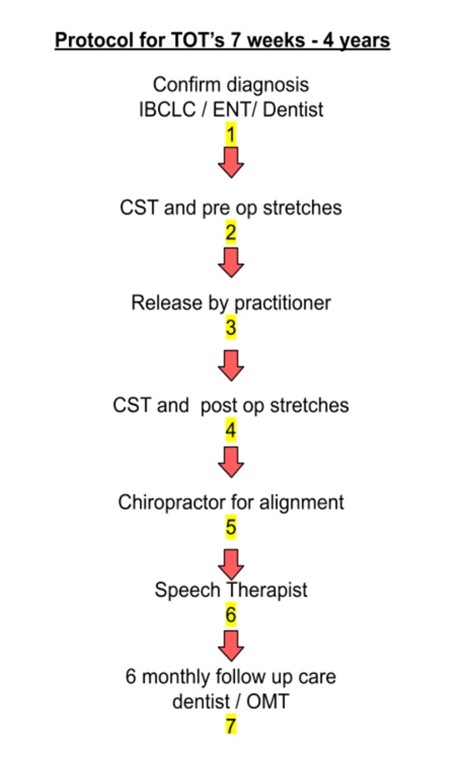
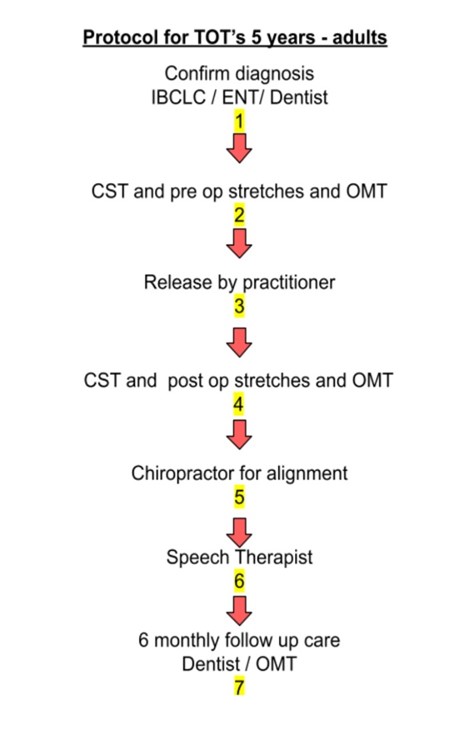
THIS IS OUR MULTI DISCIPLINARY PROTOCOL :